
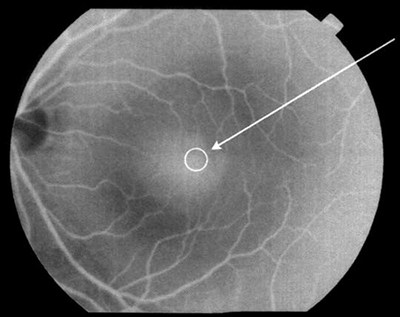
What is a macular hole?
A macular hole is a small, circular gap which opens up at the centre of the retina.
This causes blurred vision and often distorted vision where straight lines or letters look wavy or bowed. There may also be a patch of missing vision at the centre.
Is a macular hole the same as age-related macular degeneration?
No, macular holes and macular degeneration are different conditions although they affect the same area of the eye. They can sometimes both be present in the same eye.
Why does it happen?
We do not know why macular holes develop. They most often occur in people aged 60-80, and are twice as common in women as men. We are increasingly aware that it is mainly slightly long sighted people who are affected. Other causes of macular holes include severe trauma to the eye, being very short sighted (myopic), those who have had a retinal detachment or as a result of long-standing swelling of the central retina (cystoid macular oedema).
What would happen if I did not have my macular hole treated?
If untreated, there is a small chance that some macular holes can close by themselves, with improvement in vision. However, in the majority of patients the central vision will gradually get worse to a level where you are unable to read even the largest print on an eye test chart.
The condition does not affect the peripheral vision, and so you will not go completely blind from this condition.
Will my other eye be affected?
Careful examination can assess the risk of developing a macular hole in the other eye. Dr Dubey will tell you your risk but this may be from extremely unlikely to a 1 in 10 chance. It is very important to monitor for any changes in vision of your other eye, and report these to your eye specialist, GP or optician urgently.
How is it treated and how successful is it?
A macular hole can often be repaired by an operation called a vitrectomy, peel and gas.
If the hole has been present for less than a year, the operation will be successful in closing the hole in about 90% of cases.
Of these, more than 70% will be able to see two or three lines more down a standard vision chart compared to before the operation. Even if this degree of improvement does not occur, the vision is at least stabilised and many patients find that they have less distortion. In a minority of patients the hole does not close despite surgery and the central vision can continue to deteriorate; however, a second operation can still be successful in closing the hole. It is important to understand that returning to completely normal vision is not possible.
Does it matter how long I have had the macular hole if I am interested in surgery?
There is evidence that relatively early treatment (within months) gives a better outcome in terms of improvement in vision. Studies have shown, however, that vision improvement may be possible in some patients with long-standing macular holes.
What does the operation involve?
Macular hole surgery is a form of keyhole surgery performed under a microscope. 3 small cuts (1-2mm in size) are made in the white of the eye for the insertion of very fine instruments. Firstly the vitreous jelly is removed (vitrectomy), and then a very delicate layer (the inner limiting membrane) is carefully peeled off the surface of the retina around the hole to release the traction forces that keep the hole open.
The eye is then filled with a temporary gas bubble, which presses against the hole to help it seal. The bubble of gas blocks the vision whilst it is present, but it slowly disappears over a period of about 4-8 weeks.
How long does the operation take and do I need to have a general anaesthetic?
Macular hole surgery usually takes 45-90 minutes and can be done whilst you are awake (local anaesthetic), or asleep (general anaesthetic), often as a day case procedure.
Most patients opt for a local anaesthetic, which involves a numbing injection around the eye so that no pain is felt during the operation; this is supplemented with medication to reduce anxiety (sedation).
Do I have to posture face down after the operation?
The aim of face down posturing is to keep the gas bubble in contact with the hole as much as possible to encourage it to close. Whether you are required to posture, and for how long, will depend on the size of the macular hole. Generally you will need to lie face down overnight after surgery, and then adopt a reading position during the day for 3 days.
We generally recommend not to lie on your back for a period of two weeks after the surgery.
Am I able to travel after macular hole surgery?
You must not fly or travel to high altitude on land whilst the gas bubble is still in the eye (up to 12 weeks).
If ignored, the bubble will expand at altitude, causing very high pressure resulting in severe pain and permanent loss of vision.
What else should I avoid?
If you need a general anaesthetic whilst gas is in your eye, then it is vital that you tell the anaesthetist so they can avoid certain anaesthetic agents which can cause similar expansion of the bubble. None of these exclusions apply once the gas has fully absorbed. You will notice the bubble shrinking and will be aware when it has completely gone.
How much time will I need off work?
Most people will need at least two weeks off work after surgery. The amount of time off work will depend on the kind of work you do and the kind of surgery that is done. This will need to be discussed with your surgeon.
What are the potential complications of macular hole surgery?
As with any procedure there may be risks involved. However it is unlikely that you will suffer harmful effects from a macular hole operation. In a small minority of cases, the vision may end up worse than before the surgery, and there is even a very small chance of total loss of sight.
Six specific complications of macular hole surgery, which you must be aware of, are outlined below:
- Failure of the macular hole to close: This occurs in 1-2 out of 10 patients. In most circumstances, it is possible to repeat the surgery. If the hole fails to close, then the vision may be a little worse than before the surgery.
- Cataract: This means that the natural lens in the eye has gone cloudy. If you have not already had a cataract operation, you will almost certainly get a cataract after the surgery, usually within a year but it can happen very rapidly.
- Retinal detachment: The retina detaches from the back of the eye in less than 1% of patients undergoing macular hole surgery. The vast majority of retinal detachments are repairable, but further surgery is required which can potentially result in blindness.
- Bleeding: This occurs very rarely, but severe bleeding within the eye can result in blindness.
- Infection: This is also very rare, less than 1 in 1000 patients, but if it occurs it needs further treatments and can lead to blindness.
- Raised eye pressure: An increase in pressure within the eye is quite common in the days after macular hole surgery, usually due to the expanding gas bubble. In most cases it is short-lived and controlled with extra eye drops and/or tablets to reduce the pressure, preventing any harm coming to the eye. If the high pressure is extreme or becomes prolonged, there may be some damage to the optic nerve as a result. In the majority of patients, this damage does not adversely affect the vision, but some patients require long term treatment to keep the eye pressure controlled.
Will I have to take any drops or medication after the operation?
Three types of drops are usually prescribed after surgery: an antibiotic, a steroid and a pupil-dilating agent. If all is well, then the drops are reduced over the following 2-4 weeks.
If the eye pressure is raised following surgery, additional drops and/or tablets may be prescribed to treat this.
When will I need to be seen again after the surgery?
Post-operative review is usually performed the next day (or within a few days) after surgery; then 10-14 days later and, provided all is well, about 3 months later.
Will I have to get my glasses changed?
Most people will need to change their spectacle prescription at some point after surgery. This would normally be at about 3 months following the operation, after the gas bubble has gone.
Is there anything I should look out for when I get home?
If the eye becomes increasingly red, sore and sticky or you have a change of vision that you are concerned about then please contact your assessment team for advice.
You will need the Adobe Reader to view and print these documents.




